ABSTRACT
Gastrectomy is the most effective method of treating gastric cancer, but it is commonly associated with weight loss, nutritional deficiencies, and the increased risk of malnutrition due to post-surgery complications, including gastric stasis, dumping syndrome, malabsorption, and maldigestion. Malnutrition is a risk factor for postoperative complications and poor prognosis. To prevent it and guarantee a quick recovery after surgery, continuous and individualized nutrition intervention should be performed both before surgery and postoperatively. The Department of Dietetics at Samsung Medical Center (SMC) performed nutritional status assessment before gastrectomy, initial nutritional assessment within 24 hours of admission, description of therapeutic diet after surgery, nutrition counselling before discharge, and nutritional status assessment and individual nutrition counselling after 1, 3, 6, and 12 months from surgery. This is a case report of a patient who underwent gastrectomy as well as intensive nutrition intervention in SMC.
-
Keywords: Gastrectomy; Nutrition therapy
INTRODUCTION
According to 2019 National Cancer Registry statistics, cancer incidence increased 2.5 times from 1999 to 2019, with stomach cancer having the third highest incidence. The 5-year survival rate for gastric cancer increased from 43.9% in 1993- 1995 to 74.3% in 2015- 2019 [
1]. It is becoming increasingly important to reduce the side effects of stomach cancer treatment and improve quality of life.
Most gastrectomy for gastric cancer treatment resects at least 70% of the stomach, and as a result, it is difficult to take sufficient oral intake due to a decrease in gastric volume and change in the hunger and satiety system. In addition, malabsorption and maldigestion occur due to rapid intestinal transit time, pancreatic insufficiency, bacterial overgrowth, etc., which cause weight loss and nutrient deficiency, increasing the risk of malnutrition. Indeed, approximately 40% of gastrectomy patients are malnourished, and poor nutritional status after surgery is associated with an increased risk for infections and complications, prolonged hospitalization, and higher medical expenses [
2,
3].
Appropriate nutritional interventions prevent or reduce nutrition-related side effects of surgery and improve nutrition-related outcomes such as energy and protein intake and nutritional status. Counselling is the first line of nutrition intervention and improves oral intake, body weight, and quality of life. For effective nutritional intervention, individualized nutrition counselling is needed because it takes into consideration of patient preferences and specific treatment-related side effects that affect nutritional intake. Periodic follow-up during the first year after surgery is beneficial to the patient, and intensive nutrition education is suggested to be more effective in improving nutritional status, dietary intake, and quality of life than one-time education [
4,
5,
6].
This case report describes changes in body composition, dietary intake, nutritional status, and nutrition-related side effects of a patient who underwent nutrition counselling from before gastrectomy until one year after surgery. Institutional Review Board approval was obtained from SMC (approval number 2022-09-013-001).
CASE
A 52-year-old male patient underwent laparoscopic radical gastrectomy with Billroth-I anastomosis after diagnosis with gastric cancer. According to the eighth edition of the American Joint Committee on Cancer (AJCC) staging system, the stage after surgery was T1bN0M0 (stage IA). Nutritional status was evaluated before gastrectomy, and nutrition counselling was conducted five times in total until one year after surgery. To identify eating behavior, questionnaires on the eating pattern were conducted each time, and dietary intake was investigated and analyzed using the 24-hour recall method. The Patient-Generated Subjective Global Assessment (PG-SGA) was used for nutritional assessment and body composition was analyzed using Inbody 720 Bioelectrical Impedance Analyzer (BIA). Albumin and hemoglobin in the blood test were measured as nutrition-related items.
One month before surgery
The following items were investigated during the outpatient visit before surgery. Height was 175 cm, body weight was 66.8 kg, body mass index (BMI) was 21.8 kg/m2, skeletal muscle mass (SMM) was 34.3 kg, which is considered normal, and albumin and hemoglobin levels in blood were 4.0 and 14.4 g/dL respectively, both within the normal range. Our usual dietary intake was 90% or more of the energy and protein requirements being met. No special intervention was required, with a PG-SGA score of 1 point, indicating normal nutritional status. The patient was recommended to consume a balanced diet and maintain body weight and was cautioned against consuming alcohol, tobacco, traditional remedies, and dietary supplements before surgery.
During hospitalization
On the second day after hospitalization, the initial nutritional assessment was performed, body weight was 65.9 kg, and BMI was 21.5 kg/m
2, which were similar to one month before hospitalization. The PG-SGA score was 1 point, indicating that nutritional status was normal. Fasting was required on the day of surgery and the first day after surgery. A sip of water was introduced on the second day, a post-surgery semi-fluid diet on the third day, a post-surgery semi-blended diet (SBD) stage 1 on the fourth day, and post-surgery SBD stage 2 on the fifth day. The patient was discharged on the seventh day after surgery. For nutritional management, an initial nutritional assessment was performed on the first day after hospitalization, followed by a description of the therapeutic diet on the third day after surgery and nutrition counselling on the fourth day.
Table 1 shows the patient’s daily nutritional requirements and the contents of the nutrition counselling.
Table 1The daily energy and protein requirements and the contents of nutrition counselling
Table 1
|
Variables |
Descriptions |
|
The daily energy and protein requirements |
· Energy 30 kcal/CBW kg = 2,000 kcal/day |
|
· Protein 1.2 g/CBW kg = 79 g/day |
|
The contents of nutrition counselling |
· Necessity of dietary management after gastrectomy |
|
· Principles and methods of diet after surgery |
|
· Chewing well and eating small, frequently, and slowly |
|
· Dietary principles for prevention of dumping syndrome |
|
· Post-surgery diet progression and balanced nutritional intake |
|
· Beware of excessive fat intake |
|
· Information on various snacks that can be consumed as a meal replacement |
|
· Do not lie down within 2 hr after eating |
|
· Cautions for traditional remedies and dietary supplements |
One month after surgery
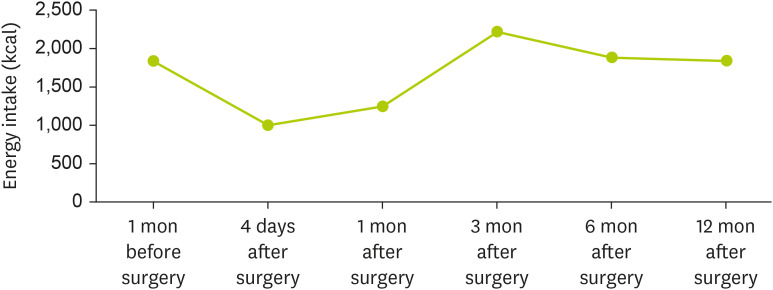
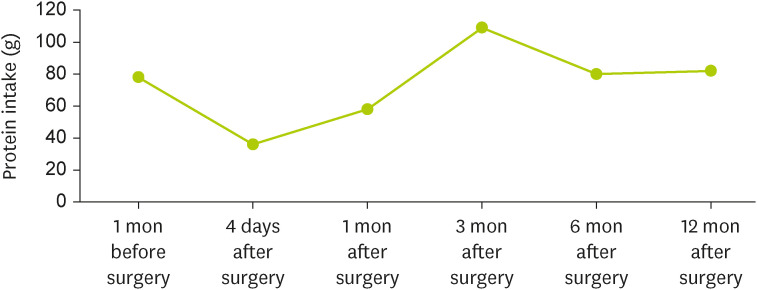
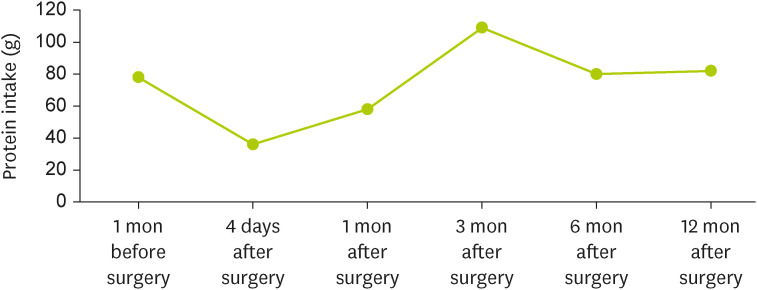
Compared to before surgery, body weight was reduced by 4.7%, SMM by 6.4%, and body fat mass (BFM) by 13.5%. Blood tests showed albumin at 4.8 g/dL and hemoglobin at 14.2 g/dL, both within normal ranges. Dietary intake was insufficient, with only 62% of the energy requirement and 73% of the protein requirement being met. The PG-SGA score was 9 points, requiring intensive nutritional intervention, and the nutritional status was moderately malnourished. The eating pattern consisted of a total of 7 eating times, including 3 meals and 4 snacks, and the time taken for each meal was about 20 to 30 minutes. The patient complained of early satiety and abdominal pain after overeating. In order to prevent dumping symptoms and reduce the frequency of pain after eating, nutrition counselling focused on maintaining meals at least 6 times and for at least 20 minutes and being careful of overeating. The patient was educated on how to transition to the general diet, avoid food, and pay attention to dietary supplements and traditional remedies.
Three months after surgery
Compared to the one month after surgery, 1.3% body weight loss and 5.8% BFM loss were observed, while SMM was similar, and blood test results were within the normal range. Energy and protein intake exceeded the requirements (111% and 138%, respectively). With a PG-SGA score of 3 points, no special nutritional intervention was required, but it was a stage in which nutritional status was maintained through counselling of the patient and caregiver, and nutritional status was normal. The eating pattern consisted of 3 meals and 5 snacks, for a daily total of 8 eating times, and the time taken for each meal was similar to the previously recorded one. After overeating, diarrhea symptoms occurred. The patient was therefore recommended to maintain the eating pattern but to beware of overeating.
Six months after surgery
Compared to one month after surgery, body weight increased by 1.4%, BFM by 16.6%, SMM was similar, and blood test results were in the normal range. The energy intake was 94% of the requirement, and the protein intake was 100% of the requirement. The PG-SGA score was 4 points, which required intervention by medical staff for symptoms related to dietary intake, but the nutritional status was normal. Diarrhea symptoms improved, but abdominal pain symptoms reappeared after overeating, and nutrition counselling was conducted the same way as 3 months after surgery.
Twelve months after surgery
Compared to 6 months after surgery, body weight increased by 3%, SMM by 3.1%, and BFM by 8.9%. Intake provided 92% energy and 102% protein requirements, a PG-SGA score of 4 points, and normal nutritional status. The eating pattern consisted of 3 meals and 6 snacks, for a total of 9 eating times, and the time taken for each meal was about 20 to 30 minutes. The amount of food per meal was reduced, and eating times increased compared to before. Previously observed abdominal pain and diarrhea symptoms after overeating improved. Nutrition counselling was completed by repeating the principles and methods of diet, maintenance of current nutritional status, prevention of dumping syndrome and digestive symptoms, and precautions.
Changes in body composition, blood test results, PG-SGA score, and dietary intake throughout the 6 nutrition counselling sessions before and after surgery are presented in
Table 2,
Figures 1, and
2.
Table 2Changes of clinical characteristics and PG-SGA score
Table 2
|
Clinical characteristics |
1 mon before surgery |
4 days after surgery |
1 mon after surgery |
3 mon after surgery |
6 mon after surgery |
12 mon after surgery |
|
Anthropometric data |
|
|
|
|
|
|
|
Body weight (kg) |
66.8 |
65.8 |
62.8 |
62.0 |
62.9 |
64.8 |
|
BMI (kg/m2) |
21.8 |
21.4 |
20.5 |
20.3 |
20.5 |
21.2 |
|
SMM (kg) |
34.3 |
- |
32.1 |
32.0 |
31.8 |
32.8 |
|
BFM (kg) |
5.9 |
- |
5.1 |
4.8 |
5.6 |
6.1 |
|
PBF (%) |
8.9 |
- |
8.1 |
7.8 |
8.8 |
9.3 |
|
Biochemical data |
|
|
|
|
|
|
|
Albumin (g/dL) |
4.8 |
4.0 |
4.8 |
4.7 |
4.1 |
4.6 |
|
Hemoglobin (g/dL) |
14.4 |
12.9 |
14.2 |
14.3 |
13.7 |
14.4 |
|
PG-SGA score |
1 |
4 |
9 |
3 |
4 |
4 |
Figure 1Change of energy intake.
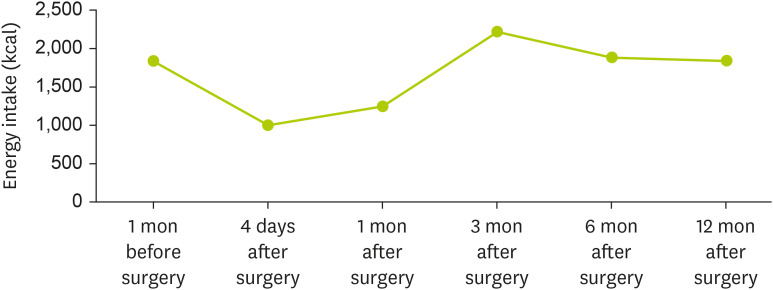
Figure 2Change of protein intake.
DISCUSSION
This case report describes changes in body composition, dietary intake, eating pattern, and nutritional status of a gastric cancer patient who underwent intensive nutritional counselling until one year after gastrectomy surgery.
After gastrectomy, problems such as the small gastric remnant, delayed gastric emptying, dumping syndrome, and diarrhea makes it difficult to obtain sufficient nutrition, leading to body weight loss and nutritional deficiencies, which increase the risk of malnutrition. Lee et al. [
5] reported that approximately 90% of patients who underwent gastrectomy lost about 5% of their body weight by 3 months after surgery. Matsushita et al. [
7] reported that body weight and BFM continued to decrease up to 12 months after gastrectomy, and body muscle mass was maintained after decreasing from 1 to 3 months after surgery, and albumin levels were lowest at 1 month and recovered after that.
The causes of weight loss and body composition change after gastrectomy are complex. Small gastric remnant caused by surgery leads to insufficient oral intake and impaired carbohydrate digestion resulting in insufficient glucose uptake, glycogen storage deficiency, and finally decreased body fat [
8]. The decrease in body muscle mass in the early stages after surgery is thought to be due to hypercatabolism caused by surgical stress and insufficient protein digestion [
9].
This case shows that body weight, SMM, and BFM improved faster than observed in other studies, which is likely to be a result of continuous nutrition counselling. Although dietary intake was insufficient to meet the nutritional requirements until 1 month after surgery, the intake was adequate from 3 months after surgery, and the nutritional status was normal. Therefore, we suggest continuous and individualized nutrition counselling after gastrectomy helps to recover nutritional status quickly and reduce and improve postoperative side effects.
NOTES
-
Conflict of Interest: The authors declare that they have no competing interests.
-
Author Contributions:
Conceptualization: Youn SY.
Data curation: Youn SY.
Formal analysis: Youn SY.
Investigation: Youn SY.
Methodology: Youn SY.
Project administration: Youn SY.
Supervision: Youn SY.
Visualization: Youn SY.
Writing - original draft: Youn SY.
Writing - review & editing: Kim BE, Kim EM.
REFERENCES
- 1. Korea Central Cancer Registry. 2019 National Cancer Registry Statistics [Internet]. 2020. cited 2021 December 29. Available from https://www.cancer.go.kr
- 2. Ryu SW, Kim IH. Comparison of different nutritional assessments in detecting malnutrition among gastric cancer patients. World J Gastroenterol 2010;16:3310-3317.
- 3. Oh CA, Kim DH, Oh SJ, Choi MG, Noh JH, Sohn TS, Bae JM, Kim S. Nutritional risk index as a predictor of postoperative wound complications after gastrectomy. World J Gastroenterol 2012;18:673-678.
- 4. Rogers C. Postgastrectomy nutrition. Nutr Clin Pract 2011;26:126-136.
- 5. Lee HO, Han SR, Choi SI, Lee JJ, Kim SH, Ahn HS, Lim H. Effects of intensive nutrition education on nutritional status and quality of life among postgastrectomy patients. Ann Surg Treat Res 2016;90:79-88.
- 6. Kenny E, Touger-Decker R, August DA. Structured review of the value added by the registered dietitian to the care of gastrointestinal cancer patients. Nutr Clin Pract 2021;36:606-628.
- 7. Matsushita H, Tanaka C, Murotani K, Misawa K, et al. Nutritional recovery after open and laparoscopic distal gastrectomy for early gastric cancer: a prospective multicenter comparative trial (CCOG1204). Dig Surg 2018;35:11-18.
- 8. Armbrecht U, Lundell L, Lindstedt G, Stockbruegger RW. Causes of malabsorption after total gastrectomy with Roux-en-Y reconstruction. Acta Chir Scand 1988;154:37-41.
- 9. Saito A, Noguchi Y, Yoshikawa T, Doi C, Fukuzawa K, Matsumoto A, Ito T, Tsuburaya A, Nagahara N. Gastrectomized patients are in a state of chronic protein malnutrition analyses of 23 amino acids. Hepatogastroenterology 2001;48:585-589.