ABSTRACT
Hemodialysis (HD) patients face a common problem of malnutrition due to poor appetite. This study aims to verify the appetite alteration model for malnutrition in HD patients through quantitative data and the International Classification of Functioning, Disability, and Health (ICF) framework. This study uses the Mixed Method-Grounded Theory (MM-GT) method to explore various factors and processes affecting malnutrition in HD patients, create a suitable treatment model, and validate it systematically by combining qualitative and quantitative data and procedures. The demographics and medical histories of 14 patients were collected. Based on the theory, the research design is based on expansion and confirmation sequence. The usefulness and cut-off points of the creatinine index (CI) guidelines for malnutrition in HD patients were linked to significant categories of GT and the domain of ICF. The retrospective CIs for 3 months revealed patients with 3 different levels of appetite status at nutrition assessment and 2 levels of uremic removal. In the same way, different levels of dry mouth, functional support, self-efficacy, and self-management were analyzed. Poor appetite, degree of dryness, and degree of taste change negatively affected CI, while self-management, uremic removal, functional support, and self-efficacy positively affected CI. This study identified and validated the essential components of appetite alteration in HD patients. These MM-GT methods can guide the selection of outcome measurements and facilitate the perspective of a holistic approach to self-management and intervention.
-
Keywords: Appetite; Mixed methods research; Hemodialysis; Self-management; International Classification of Functioning, Disability and Health (ICF)
INTRODUCTION
Malnutrition is a common problem among hemodialysis (HD) patients, and it can have a substantial influence on their quality of life and overall health outcomes. Appetite alterations are a major cause of malnutrition in this population, and effective self-management strategies that incorporate a holistic approach are required to address this issue [
1]. A holistic approach to self-management takes into consideration not only the physical elements of malnutrition but also the psychological, social, and cultural factors that may influence an individual’s nutrition and health. Patients undergoing HD can improve their nutritional status, improve their quality of life, and lower their risk of malnutrition-related health problems by using a comprehensive, holistic approach to self-management. Although there are disease-specific markers and recommendations for malnutrition, overall nutrition management requires systematic and holistic intervention.
The Nutrition Care Process (NCP) is a standardized approach to providing quality nutrition care to individuals and populations [
2]. The NCP is based on the use of 2 internationally recognized frameworks, the International Dietetics and Nutrition Terminology (IDNT) and the International Classification of Functioning, Disability, and Health (ICF) [
3]. In NCP practice, either ICF from World Health Organization (WHO) or IDNT from the USA is generally used [
4]. Lately, the profession has adopted the ICF as a framework for approaching patient care, shifting the conceptual emphasis away from negative connotations such as disability and focusing on the positive abilities of the individual at the patient level rather than the system level. The ICF framework is a classification of health components of functioning and disability that focuses on 3 perspectives: body, individual, and social. These 3 approaches emphasize the significance of the interaction and effect of both internal and environmental influences on each individual’s health. To map outcomes across domains, the ICF was employed. The most prevalent patient-centered outcome measure was health-related quality of life [
5].
Throughout this approach, the dietician focused on outcomes and measurements when choosing appropriate outcome measures to assess progress across all areas of ICF. They evaluated the effectiveness of treatment from a holistic and patient-centered perspective [
6]. The ICF was chosen as a widely recognized, comprehensive biopsychosocial framework reference point to guide this study. The ICF Core Sets are shortlists of ICF codes related to health issues that span life. The ICF-Dietetics was chosen as a widely recognized, comprehensive biopsychosocial framework reference point to guide this study. The ICF Core Sets are shortlists of the ICF codes related to health issues that span life. The ICF-Dietetics [
7] is particularly relevant to this study because it intends to provide adequate care and support for HD patients.
IDNT and ICF-Dietetics are based on different methodologies within the NCP process. But the 2 methods could harmonize the common characteristics of these various nutritional and dietary terms, especially within the concept of evaluation, diet diagnosis, and evaluation. However, ICF-Dietetics would be more advantageous in terms of multidisciplinary application [
3]. Nevertheless, a paradigm change from medical diagnosis-focused health care to a holistic perspective of functioning with a greater emphasis on Participation and Environmental Factors is needed for the successful adoption of the ICF-Dietetics in clinical practice [
7].
The ICF-Dietetics implementation allows for a holistic view of functioning with attention to participation and environmental factors, which have been overlooked in traditional nutritional care management [
8]. The ICF-Dietetics is not used by most hospitals in Korea, although it is used in several hospitals in Europe and Australia [
4]. In order to deliver excellent nutritional care in rehabilitation, NCP and the ICF are used [
9]. Body function plays a significant role for dietary services in HD and rehabilitation patients, as well as participation and environmental factors. The bodily impairment that affects appetite alteration due to uremic conditions are applied as a component of body function in HD patients.
Studies using Mixed Method-Grounded Theory (MM-GT) are becoming more prevalent. Major MM professional associations, such as the Mixed Method Special Interest Group of the American Educational Research Association’s Mixed Method Special Interest Group and the Mixed Method International Research Association, have also acknowledged the quality of methodological rigor in addition to the growing number of MM-GT papers [
10].
The exploratory–confirmatory MM-GT design requires systematic study to the context of discovery and the context of justification. The discovery context is primarily inductive, starts with local data, and attempts to find or construct a theory. The justificational context focuses on reasoning of scientific knowledge through theory and hypothesis testing. In order to create a more insightful and well-supported comprehensive whole, MM-GT studies methodically combine a significant purpose of qualitative research (i.e., inductive theory construction) with a primary purpose of quantitative research (i.e., empirically testing theoretical relationships). This confluence of rationales and efforts makes the MM-GT design a robust design. An excellent explanatory theory may be created using the MM-GT research method, which depends on using qualitative, quantitative, and MMs data, procedures, logical reasoning, and strategies [
11]. This study is a method of mixing qualitative and quantitative data based on the MM-GT method. We want to explore various factors and processes affecting malnutrition, create a suitable treatment model for HD patients, and research to validate these models systematically.
This study is the last of a series of studies on the nutritional management of malnutrition in HD patients. The initial study developed a malnutrition screen tool for HD patients as a quantitative study. Subsequently, the appetite alteration model was created to explain the process and factors by exploring the unique malnutrition state due to poor appetite through qualitative research. Finally, we would like to verify this model using quantitative data. The universally recognized ICF, approved by WHO, is a biopsy-psychosocial framework and has been used as a reference point for testing content validity. We will establish the content validity of the identified domain using evidence theory and comparability with categories within ICF-Dietetics. This study aimed to identify and verify the theoretical area of the appetite alteration model and to provide information on the development of a person-centered outcome measurement framework.
MATERIALS AND METHODS
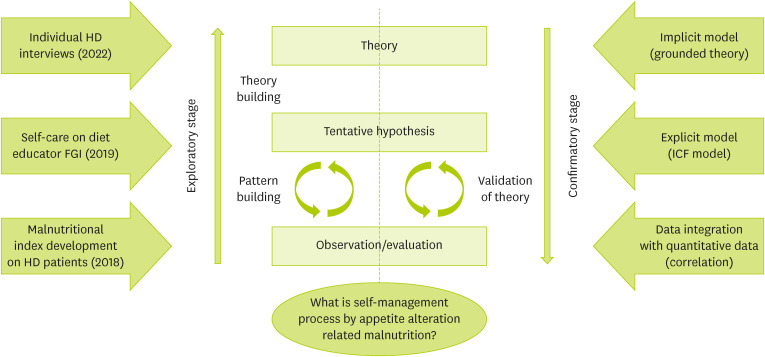
This study presents a complex research design of continuous research results, as shown in
Figure 1. The previous study began in 2013 to take nutritional diagnoses for HD patients using IDNT in a single tertiary center. IDNT was applied to HD patients, and the correlations of the IDNT results to other clinical parameters were studied. IDNT was an effective diagnostic tool for HD patients [
12]. However, most current nutritional evaluation methods are subjective, time-consuming, and cumbersome. Therefore, convenient and simple tools are needed for early and individualized malnutrition screening and determining the outcomes after appropriate intervention in HD patients. Before this study, an examination of a nutrition screening tool for HD patients [
13] and a qualitative study of self-care through dynamic appetite alteration [
1] was conducted in the HD unit of Ajou University Hospital. This study used an MM-GT exploratory instrument development design in
Figure 1.
Figure 1
Overall structure of the study.
HD, hemodialysis; ICF, International Classification of Functioning, Disability, and Health; FGI, focus group interview.
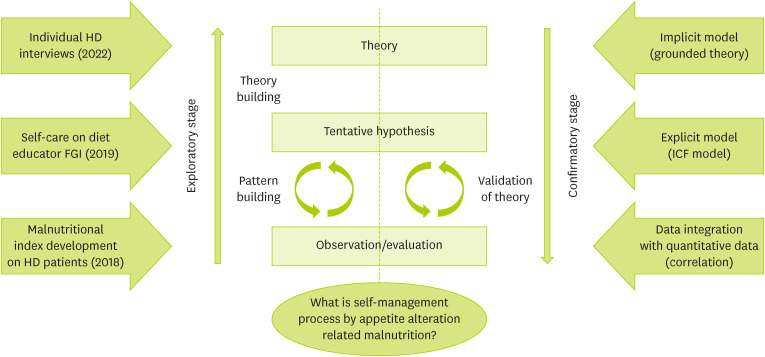
This study used multiple methods, which is a research program of quantitative study 1 [
13] and qualitative study 2 [
1]. Study 1 and study 2 are related but thoroughly independent studies. Furthermore, study 2 is the mixed-methods design, a single research study with a complete method and a component of another. Study 1 used to make nutrition screen tools for malnourished HD patients using creatinine Index (CI) in 2014 with the same HD patients [
13]. However, the nutrition screen tool did not include appetite, which is a crucial factor in malnutrition. Study 2 is to understand the appetite experienced by HD patients and how to adjust them. Measuring the appetite of HD patients is not a suitable tool, and objectively measuring patients with chronic diseases is challenging. Qualitative research for HD patients will be studied. We conducted a complex MMs study, conceptualizing the qualitative strands as a GT approach. By gathering and evaluating both closed-ended and open-ended data in an integrated manner, the MM concept merges the 2 major paradigms of quantitative and qualitative research into a single study [
14].
Results were synthesized using clinical statistics and categories from selective coding where appropriate. For outcome data, 2 reviewers familiar with the ICF (Hwang W and Lee JH) used published linking rules to map outcomes to the ICF [
3]. Meaningful concepts for each measure and component were identified and linked to the most precise category using the ICF browser [
15]. Agreement on these interpretations was reached via discussion, including decisions regarding whether a measure was related to activity or participation, using operational definitions [
6].
In these previous studies, we performed in-depth, face-to-face, individual interviews with the same HD patients to examine patient perspectives about appetite and taste. All patients were older than 18 and had been on maintenance HD treatment for at least 3 months. Purposive sampling was used to choose HD patients for the study. We chose patients for this study until we reached the data saturation threshold from 80 participants who got nutritional care services. Fourteen patients were ultimately included in our sample. Before the interview, each participant signed a formal agreement of informed consent. The Ajou University Medical Center’s Institutional Review Board approved the study procedures (AJIRB-MED-SUR-17-138). Demographics and medical histories were reviewed; dialysis treatment parameters such as dialysis vintage, age, and interdialytic weight gain (IDWG). Nutritional markers, such as albumin and CI, were determined. All predialysis blood samples were obtained for routine monthly laboratory assessment using standard techniques. The simple formula for CI prediction calculated from dialysis dosage and HD patient demographics was developed via mixed regression models [
13]. Repeated measures analysis of variance was conducted in CI using a general linear model of components in ICF for grouping over 4 months before nutritional assessment. Nonparametric Kruskal-Wallis and Mean-Whitney U were used to examine differences among the study variables according to core categories from the GT approach. Duncan post hoc analysis was conducted to identify the specific groups that led to a significant difference. Spearman correlation analysis was used to check multicollinearity and assumption for the hypothetical model. Statistical analyses were performed with SPSS version 22.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
ICF model framework
In study 2, selective coding in GT research was used to identify the self-care process related to appetite as the core category. These properties were sensitivity of urea removal, degree of taste alteration, types of functional supports, levels of knowledge and self-efficacy, and degree of self-monitoring. During search reconstruction, the levels of knowledge and self-efficacy ranged from low to high, and the degree of self-monitoring ranged from partial to overall. A detailed description of each category can be found in the other publications [
1]. The following framework, displayed below (
Figure 1), illustrates our research design’s exploratory, confirmatory sequence. The overarching GT construct is supported by an initial pattern and tentative theory construction, and at the time of theoretical saturation, it experiences a change from exploratory to confirmatory. From there on out, the emerging theory undergoes methods of validation.
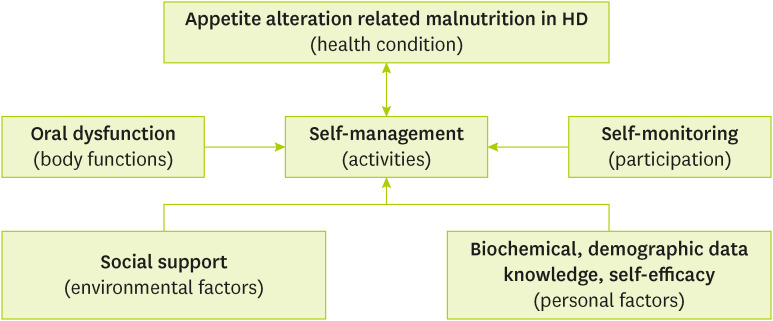
The indices indicated a good fit for the hypothetical model in
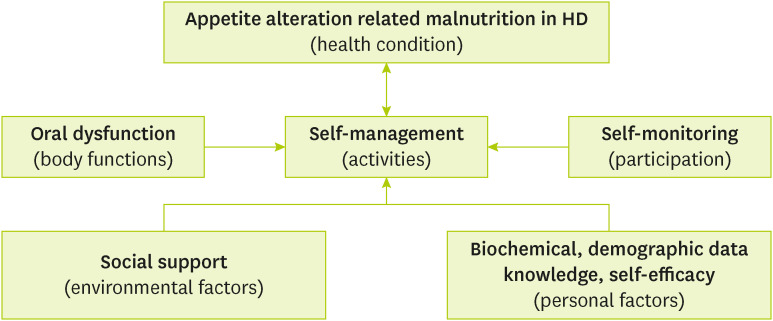
Figure 2. This model integrates the ICF framework into the self-care process using the appetite alteration model related to malnutrition context as a structural base.
Figure 2 illustrates how the dietitians utilized the evaluation for the nutritional status of HD patients with poor appetite. Using the structure provided by the tool and identifying patient problems within the context of the ICF has the advantage of not only considering one-dimensional factors but also reflecting various factors for the dietitians, which are the most important to the patients. These factors include formulating a self-care process and identifying other resources (i.e., social support) to help manage some factors outside the typical scope of nutritional therapy. The dietitians were also able to identify personal factors that could be a facilitator or barrier to the patient’s overall progress. By doing this, the dietitians accentuated the facilitators (self-efficacy) and the barriers (oral dysfunctions) to help patients achieve their goals as quickly as possible. Considering the relationship among components in the ICF model, self-management was negatively related to poor appetite in malnutrition. There were several environmental factors and personal factors that were positively related to self-management. Sensitivity of uremic removal in oral dysfunction, self-monitoring in participation, and functional support in the environmental factors were positive relations with self-management. For the personal factors, self-efficacy, albumin level, and CI were positive relations with self-management.
Figure 2
An adapted International Classification of Functioning, Disability and Health model used to explore the associations among components related to appetite alteration model in HD patients.
HD, hemodialysis.
Patient characteristics and longitudinal changes in CI according to ICF components
A total of 15 HD patients enrolled, and 14 patients (93%) participated after one participant withdrew due to a newly discovered health issue. The mean age and HD vintage of the participants was 60 (40–80) and 5.8 (0.5–13) years. The participants were almost female (64%), and 2 participants had diabetes. The 2 participants were on HD again after a kidney transplant due to rejection. One participant underwent HD again due to failure of peritoneal dialysis.
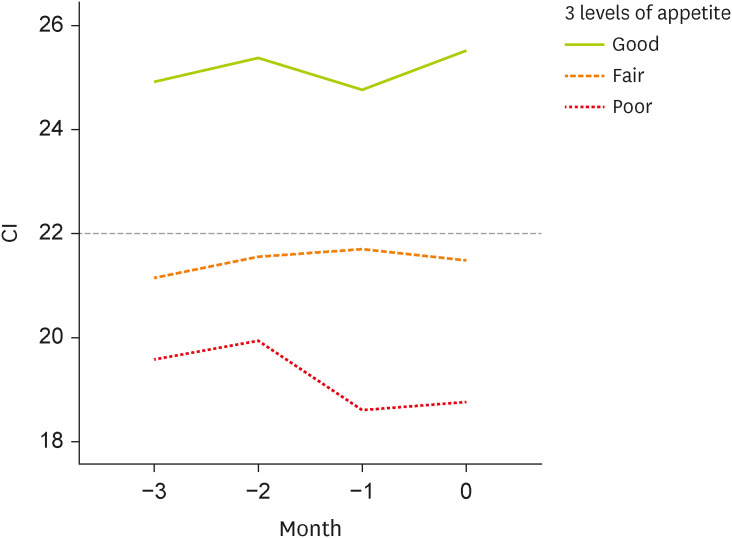
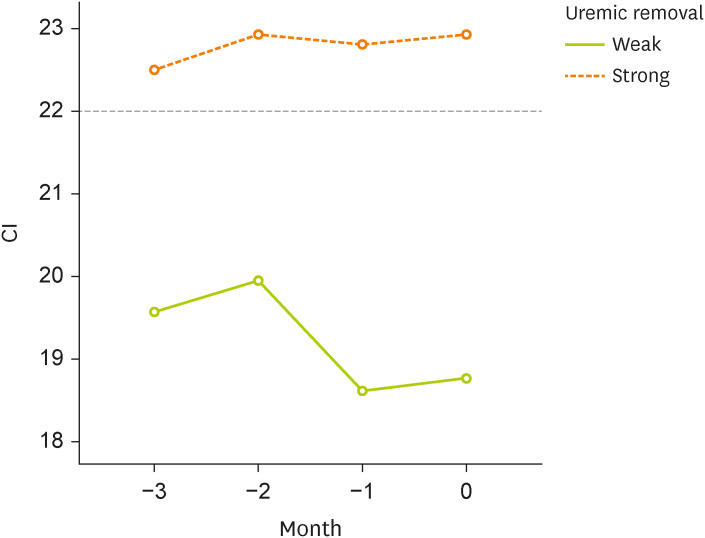
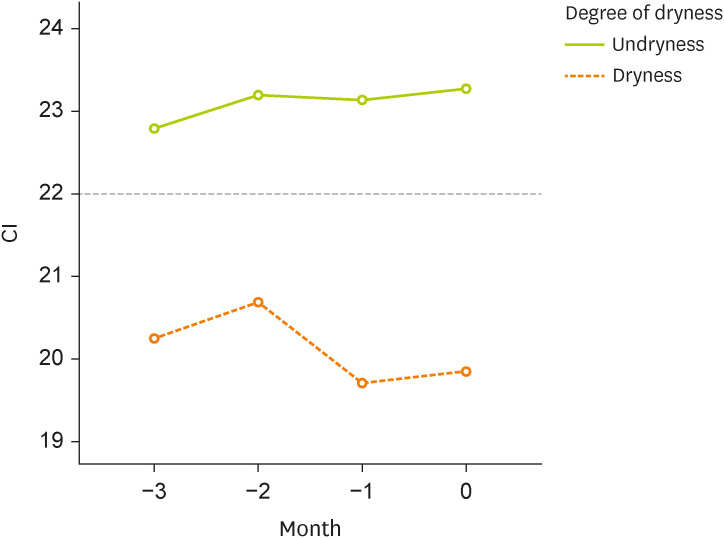
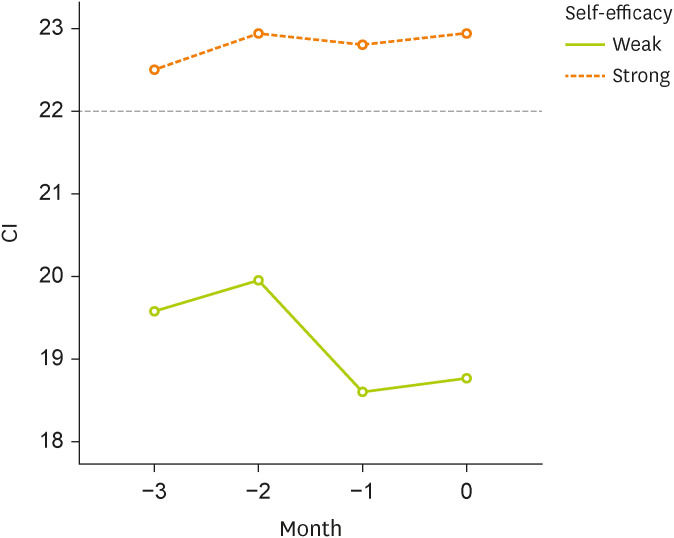
CI showed an optimal cut-off of < 22 in predicting malnutrition [
13]. Based on the time of nutritional assessment, different levels of each factor were shown in
Figures 3-
8. The retrospective CIs for 3 months revealed patients with 3 different levels of appetite status at nutrition assessment (
Figure 3, p = 0.007) and 2 different levels of uremic removal (
Figure 4, p = 0.011). In the same way, different levels of dry mouth (
Figure 5, p = 0.042), functional support (
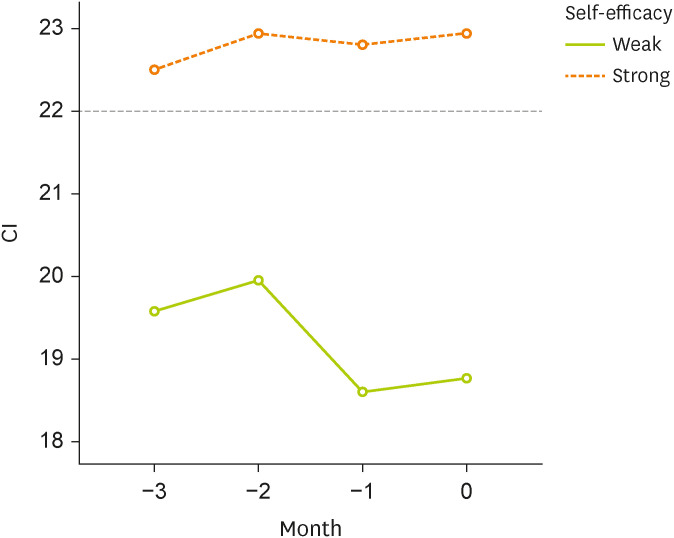
Figure 6, p = 0.014), self-efficacy (
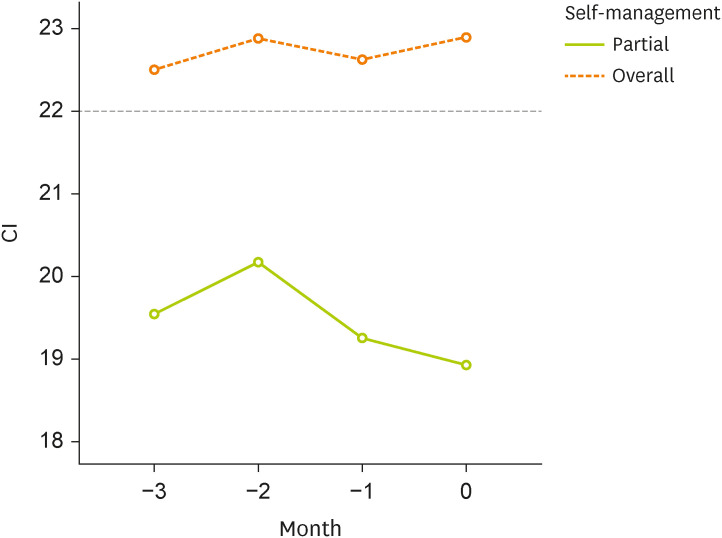
Figure 7, p = 0.011), and self-management (
Figure 8, p = 0.022) were analyzed.
Figure 3
Changes in CI based on appetite levels over 3 months.
CI, creatinine index.
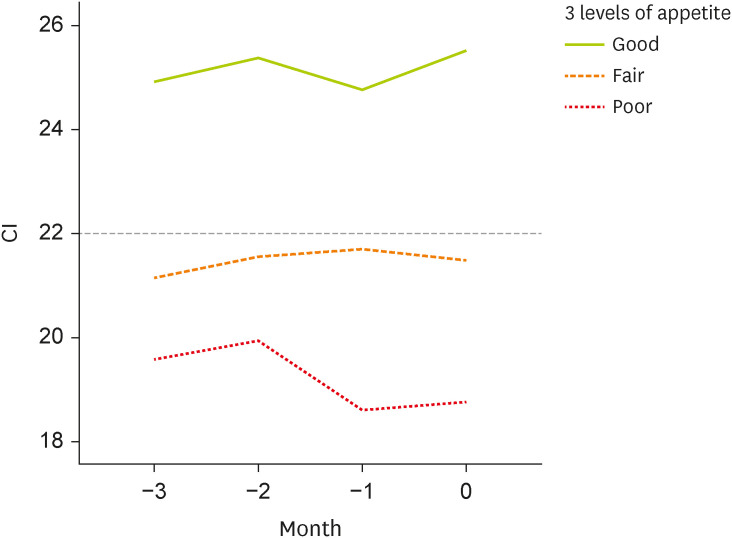
Figure 8
Changes in CI based on self-management levels over 3 months.
CI, creatinine index.
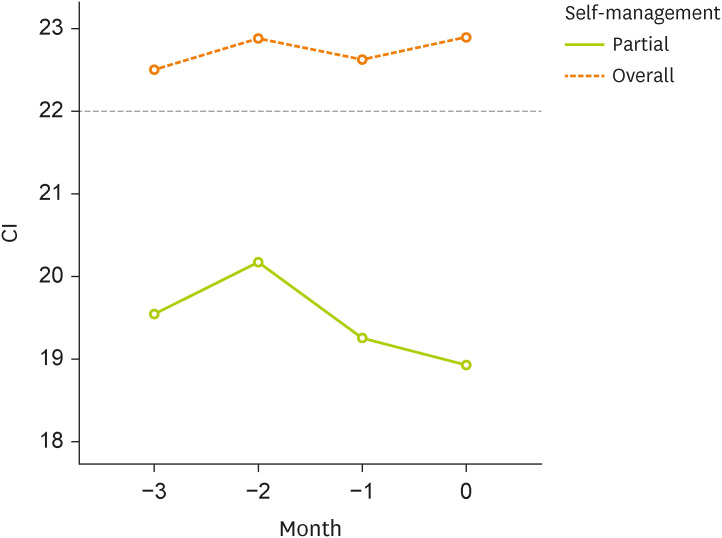
Figure 4
Changes in CI based on sensitivity over 3 months.
CI, creatinine index.
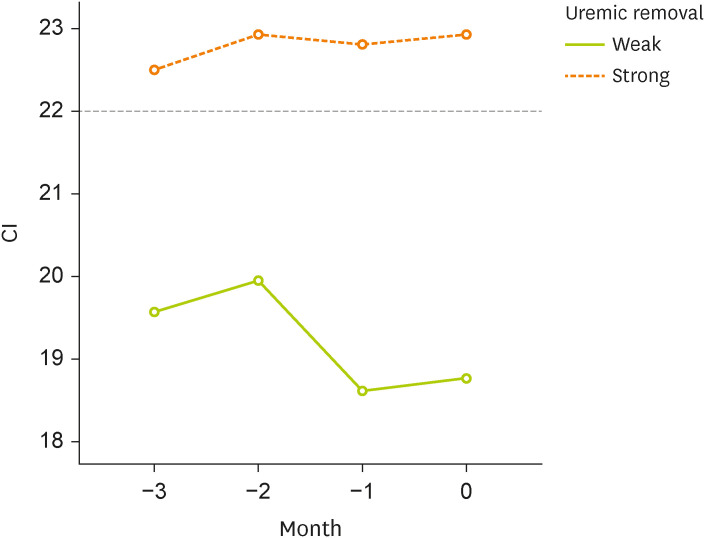
Figure 5
Changes in CI based on degree of dry mouth over 3 months.
CI, creatinine index.
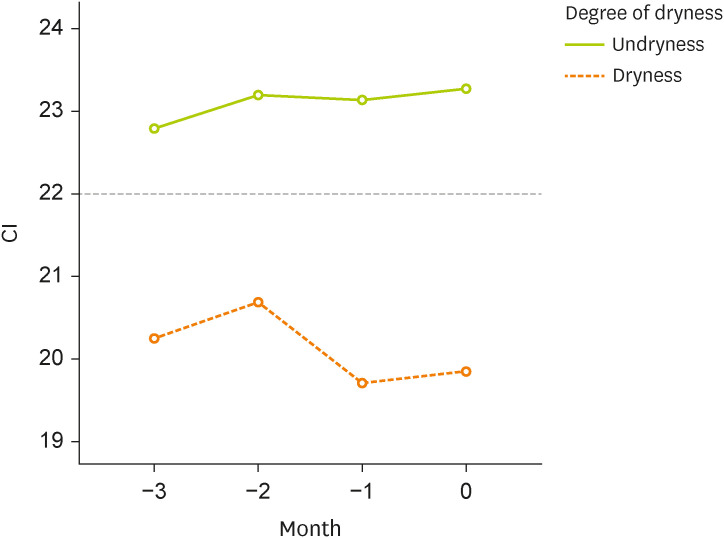
Figure 6
Changes in CI based on functional social support groups over 3 months.
CI, creatinine index.
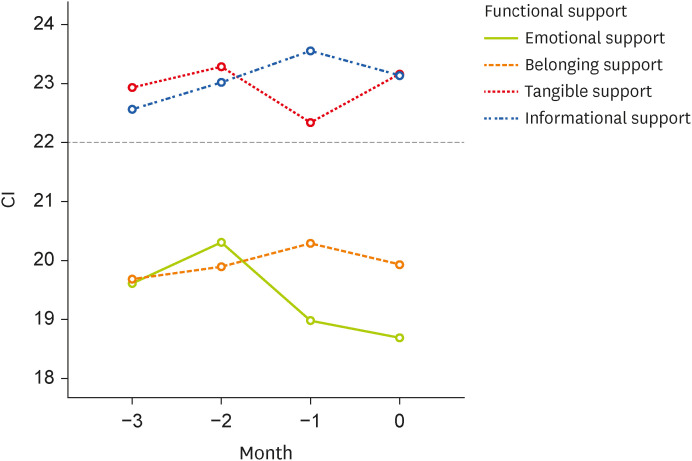
Figure 7
Changes in CI based on self-efficacy levels over 3 months.
CI, creatinine index.
Clinical indices and ICF components
Table 1 shows the correlation of components with personal factors in ICF. Poor appetite, degree of dryness, and degree of taste change were negatively associated with CI. Also, self-management, uremic removal, functional support, and self-efficacy were positively associated with CI. The older the age, the greater the degree of taste change. On the contrary, self-management, natural removal, functional support, and self-efficiency decreased with age. The longer the period of dialysis, the less appetizing it was. The longer the dialysis period, the greater the degree of dryness, taste change, and knowledge, but the less uremic remission and self-efficiency. IDWG was negatively associated with the predialysis uremic condition.
Table 1Correlation among appetite, oral condition, self-management, social support, self-monitoring and demographics and biochemical parameters
Table 1
|
Spearman rho |
HC |
A |
P |
BF |
EF |
PF |
|
ICF |
Category |
Poor appetite |
Self-management |
Self-monitoring |
Predialysis uremic |
Uremic sensitivity |
Degree of dryness |
Degree of taste change |
Functional support |
Knowledge |
Self-efficacy |
Age |
Dialysis vintage |
IDWG |
Alb |
CI |
|
HC |
Poor appetite |
1.000 |
−0.576*
|
−0.576*
|
0.330 |
−1.000†
|
0.701†
|
0.701†
|
−0.440 |
0.330 |
−1.000†
|
0.651*
|
0.713†
|
−0.367 |
−0.497 |
−0.669†
|
|
A |
Self-management |
|
1.000 |
0.576*
|
−0.330 |
0.576*
|
−0.337 |
−0.337 |
0.826†
|
0.055 |
0.576*
|
−0.542*
|
−0.324 |
0.259 |
0.627*
|
0.626*
|
|
P |
Self-monitoring |
|
|
1.000 |
0.055 |
0.576*
|
−0.337 |
−0.337 |
0.440 |
−0.330 |
0.576*
|
−0.477 |
−0.453 |
−0.108 |
0.195 |
0.324 |
|
BF |
Predialysis uremic |
|
|
|
1.000 |
−0.330 |
0.471 |
0.471 |
−0.050 |
0.300 |
−0.330 |
0.059 |
0.353 |
−0.746†
|
−0.196 |
−0.392 |
|
Uremic sensitivity |
|
|
|
|
1.000 |
−0.701†
|
−0.701†
|
0.440 |
−0.330 |
1.000†
|
−0.651*
|
−0.713†
|
0.367 |
0.497 |
0.669†
|
|
Degree of dryness |
|
|
|
|
|
1.000 |
0.689†
|
−0.189 |
0.471 |
−0.701†
|
0.520 |
0.832†
|
−0.370 |
−0.592*
|
−0.573*
|
|
Degree of taste Δ |
|
|
|
|
|
|
1.000 |
−0.189 |
0.471 |
−0.701†
|
0.687†
|
0.684†
|
−0.592*
|
−0.592*
|
−0.536*
|
|
EF |
Functional support |
|
|
|
|
|
|
|
1.000 |
0.300 |
0.440 |
−0.689†
|
−0.157 |
0.137 |
0.471 |
0.667†
|
|
PF |
Knowledge |
|
|
|
|
|
|
|
|
1.000 |
−0.330 |
0.059 |
0.784†
|
0.059 |
0.000 |
0.196 |
|
Self-efficacy |
|
|
|
|
|
|
|
|
|
1.000 |
−0.651*
|
−0.713†
|
0.367 |
0.497 |
0.669†
|
|
Age |
|
|
|
|
|
|
|
|
|
|
1.000 |
0.468 |
−0.309 |
−0.551*
|
−0.755†
|
|
Dialysis vintage |
|
|
|
|
|
|
|
|
|
|
|
1.000 |
−0.128 |
−0.442 |
−0.319 |
|
IDWG |
|
|
|
|
|
|
|
|
|
|
|
|
1.000 |
0.319 |
0.605*
|
|
Alb |
|
|
|
|
|
|
|
|
|
|
|
|
|
1.000 |
0.488 |
|
CI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1.000 |
DISCUSSION
This study gave insight into patients’ experiences living with appetite alteration after HD treatment. Our findings suggest that applying the MM-GT research method to the ICF frame verified the self-management process by appetite alternation theory. Our study provides a conceptual basis for a person-centered measurement framework of malnutrition, oral dysfunction, self-care, social support, and personal factors that can be operationalized within HD settings and complement the ICF. By understanding gaps in the ICF and broadening the measurement scope in HD care, we can measure the biological state of health and what matters to individuals about their support and internal factors.
Focusing on a single condition or outcome is less valuable than using a person-centered approach to measuring [
16]. The domains and concepts we discovered collectively offer a balanced biopsychosocial view of HD patients. This view is constructive in the area of NCP, as HD patients frequently use a combination of social and nutritional care services, where a lack of adequate outcome indicators may undervalue the scope of services offered. While clinical indicators are essential to guarantee the quality and safety of treatment for HD patients, care providers should complement them with measurements that capture many important aspects of the overall NCP. Intrinsic personal characteristics and environmental factors should be assessed as part of person-centered and comprehensive outcomes measuring methodology outcome [
16].
MM-GT may be used in various fields, settings, and contexts. MM-GT may be a good resource for creating a theory, model, or framework. Grounded theorists benefit considerably from MM-GT when using MMs designs, as do MMs researchers who prefer GT to alternative qualitative approaches [
17]. Verifying the model made in consideration of factors affecting malnutrition due to poor appetite in HD patients with quantitative data can commonly be applied in the clinical nutrition field.
The study’s principal weakness is the small sample size of people treated in a single tertiary HD unit. These findings may not apply to all HD patients. Notwithstanding the limited number of patients polled, the findings of this study give fresh insights into clinical nutrition management as a foundation for understanding HD patient situations and attitudes regarding the disease process [
18]. In addition, it is the first case of applying a current research method.
We suggest that researchers interested in applying MM-GT start by reviewing the literature on MMR and GT, getting training, and looking for a mentor to offer guidance. It is essential to understand the components of each approach and consider design possibilities if dietitians want to lead the research process. Most importantly, we recommend adding more insights to findings to aid the multidisciplinary research area in understanding both the research methods (such as MMs integration) and the results (such as theory generated from GT analysis) [
17]. We hope these MM-GTs will be applied to clinical educators who conduct research with clinical dietitians who manage patients in the clinical field to contribute to revealing the effectiveness of NCP.
NOTES
-
Conflict of Interest: The authors declare that they have no competing interests.
-
Author Contributions:
Conceptualization: Hwang W, Oh J, Park I, Cho MS.
Data curation: Hwang W, Lee JH.
Investigation: Hwang W, Cho MS.
Writing - original draft: Hwang W, Ahn SE.
Writing - review & editing: Hwang W, Lee JH, Ahn SE, Guak J, Oh J, Park I, Cho MS.
REFERENCES
- 1. Hwang W, Lee JH, Nam J, Oh J, Park I, Cho MS. Self-care through dynamic appetite alteration: a grounded theory study of patient experience on maintenance hemodialysis. Clin Nutr Res 2022;11:264-276.
- 2. Lewis SL, Miranda LS, Kurtz J, Larison LM, Brewer WJ, Papoutsakis C. Nutrition care process quality evaluation and standardization tool: the next frontier in quality evaluation of documentation. J Acad Nutr Diet 2022;122:650-660.
- 3. Gäbler G, Coenen M, Fohringer K, Trauner M, Stamm TA. Towards a nationwide implementation of a standardized nutrition and dietetics terminology in clinical practice: a pre-implementation focus group study including a pretest and using the consolidated framework for implementation research. BMC Health Serv Res 2019;19:920.
- 4. Alkhaldy AA, Allahyani MN, Alghamdi NA, Jeddawi AK, Malibary RM, Al-Othman AM. Status of nutrition care process implementation in hospitals in Jeddah, Saudi Arabia. Clin Nutr ESPEN 2020;36:53-59.
- 5. Hurst H, Young HM, Nixon AC, Ormandy P, Brettle A. scoping review author collaborative for outcomes and care priorities for older people with ACKD. Outcomes and care priorities for older people living with frailty and advanced chronic kidney disease: a multi-professional scoping review. Age Ageing 2022;51:afac296.
- 6. Atkinson HL, Nixon-Cave K. A tool for clinical reasoning and reflection using the international classification of functioning, disability and health (ICF) framework and patient management model. Phys Ther 2011;91:416-430.
- 7. Gäbler G, Lycett D, Gall W. Integrating a new dietetic care process in a health information system: a system and process analysis and assessment. Int J Environ Res Public Health 2022;19:2491.
- 8. Gäbler G, Coenen M, Lycett D, Stamm T. Towards a standardized nutrition and dietetics terminology for clinical practice: an Austrian multicenter clinical documentation analysis based on the International Classification of Functioning, Disability and Health (ICF)-Dietetics. Clin Nutr 2019;38:791-799.
- 9. Mizuno S, Wakabayashi H, Wada F. Rehabilitation nutrition for individuals with frailty, disability, sarcopenic dysphagia, or sarcopenic respiratory disability. Curr Opin Clin Nutr Metab Care 2022;25:29-36.
- 10. Howell Smith MC, Babchuk WA, Stevens J, Garrett AL, Wang SC, Guetterman TC. Modeling the use of mixed methods–grounded theory: developing scales for a new measurement model. J Mixed Methods Res 2020;14:184-206.
- 11. Shim M, Johnson B, Bradt J, Gasson S.. A mixed methods-grounded theory design for producing more refined theoretical models. J Mixed Methods Res 2021;15:61-86.
- 12. Kang E, Hwang W, Shin G, Kim H, Park I. Nutritional diagnosis in chronic hemodialysis patients using International Dietetics and Nutritional Terminology (IDNT). Seoul: World Congress of Internal Medicine; 2014.
- 13. Hwang W, Cho MS, Oh JE, Lee JH, Jeong JC, Shin GT, Kim H, Park I. Comparison of creatinine index and geriatric nutritional risk index for nutritional evaluation of patients with hemodialysis. Hemodial Int 2018;22:507-514.
- 14. Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. 3rd ed. Thousand Oaks: SAGE; 2018.
- 15. World Health Organization. International classification of functioning, disability and health: ICF. Geneva: World Health Organization; 2001.
- 16. Taylor S, Walton R, Martini A. Health, well-being and quality of life in aged care: Validation of theoretical domains to inform a person-centred outcomes measurement framework. Australas J Ageing 2023;42:9-19.
- 17. Guetterman TC, Babchuk WA, Smith MC, Stevens J. Contemporary approaches to mixed methods-grounded theory research: a field-based analysis. J Mixed Methods Res 2019;13:179-195.
- 18. Stevenson J, Tong A, Gutman T, Campbell KL, Craig JC, Brown MA, Lee VW. Experiences and perspectives of dietary management among patients on hemodialysis: an interview study. J Ren Nutr 2018;28:411-421.