ABSTRACT
Antioxidant compounds can attenuate inflammation and delay degenerative processes especially in the cardiovascular system. This study aimed to determine the relationship between dietary total antioxidant capacity (DTAC) and serum biomarkers in patients undergoing coronary artery bypass graft surgery. In this cross-sectional study, 146 patients who had referred to Imam Ali Hospital in Kermanshah were recruited and demographic, anthropometric, physical activity and dietary data were collected. Fasting blood glucose (FBG), serum levels of lipid profile, inflammatory markers (interleukin [IL]-17, intercellular and vascular cell adhesion molecules [ICAM, VCAM]), and total antioxidant capacity (TAC) were also measured. A regression model adjusted for confounding variables presented that the coefficients of ICAM and VCAM (ng/dL) in the third tertile of DTAC were lower than those in the first tertile (β = −417.2, 95% confidence interval [CI] = −509.9 to −324.5, p < 0.001; β = −293.2, 95% CI = −334.3, −252.1, p < 0.001, respectively). The β of serum TAC (ng/dL) in the third tertile was 0.86 (95% CI = 0.77, 0.95, p < 0.001) higher than that in the first tertile. DTAC had no statistically significant relationship with lipid profile, FBG, and IL-17 levels, and anthropometric indices. In this study DTAC was associated with increased serum TAC and decreased cell adhesion molecules. Therefore, diet antioxidants may be beneficial in attenuating of inflammation in coronary artery diseases.
-
Keywords: Coronary artery bypass; Diet; Antioxidants; Interleukin-17; Cell adhesion molecules
INTRODUCTION
Cardiovascular diseases (CVDs) are the leading cause of death in the world; over 17.5 million people die annually from CVDs, which was accounted 31% of all deaths [
1]. Dietary compounds have recently been shown as the effective factors in development or prevention of atherosclerosis [
2]. The diet containing high amounts of antioxidants is effective in preventing CVDs and their side effects [
3,
4]. To report the amount of antioxidants received from the diet, the dietary total antioxidant capacity (DTAC) was introduced as a diet index [
5,
6].
Studies have shown the effect of DTAC on attenuating of interleukin (IL)-17 and cell adhesion molecules [
7]; IL-17 increases the incidence of acute coronary syndrome by destabilizing of vascular plaques [
8,
9]. Intercellular adhesion molecule (ICAM) and vascular cells adhesion molecule (VCAM) are increased during inflammatory responses particularly in the atherosclerotic processes that can be considered as an indicator of endothelial inflammation or the onset of atherosclerosis [
10,
11]. The amounts of these molecules that are closely related to C-reactive protein (CRP), can predict the onset of heart attacks and death [
10,
11]. Circulating levels of cell adhesion molecules are lower in individuals with diets rich in fruits, vegetables, and whole grains, due to their contents of fiber and antioxidants [
12]. Serum antioxidants can convert free radicals into their inactive forms; therefore, they have anti-inflammatory effects and are associated with a lower risk of CVDs [
13,
14].
Invasive treatments including the coronary artery bypass graft (CABG) surgery may give rise to inflammatory responses, and systemic inflammation can cause atrial and ventricular arrhythmias, heart attacks, strokes, and eventually death [
15]. Regarding the effective role of diet on the inflammatory status, the present study was carried out to determine the relationship between the DTAC and serum levels of IL-17 and cell adhesion molecules in patients undergoing CABG surgery.
MATERIAL AND METHODS
Participants
In this cross-sectional study, the statistical population was all registered candidates for CABG surgery. The individuals were selected by available sampling method among the clients of Imam Ali Hospital, Kermanshah, Iran. The sample size was estimated to be at least 42 subjects based on the study of Kolarzyk et al. [
16], however to increase the accuracy of estimation, 150 eligible patients were included in the study. The inclusion criteria were patients under 80 years with clogged arteries who needed the CABG surgery based on the physician's diagnosis and angiography results. Also, the calorie intakes of eligible participants were between 2,000 and 3,000 kcal per day.
Patients with liver disorders (i.e., hepatitis, cirrhosis, and gallstones), kidney stones, pulmonary infection, diabetes, cancer, malabsorption, thyroid disorders, heart attacks and strokes or surgical history in previous six months were excluded. Also, candidates consuming drugs (i.e., aspirin, warfarin, clopidogrel, and immunosuppressive drugs, corticosteroids) and dietary supplements (i.e., antioxidants) in a month before the study were excluded. Other exclusion criteria were unwillingness to continue or failure to have the surgery for any reason.
According to the basic principles of the Helsinki Declaration, the objectives of the study were explained for the candidates and an informed written consent was obtained from each participant. This study was approved by Kermanshah University of Medical Sciences, Kermanshah, Iran (ethics code: IR.KUMS.REC.1398.1113).
Data collection
The data were collected using appropriate questionnaires including demographic questionnaire, food frequency questionnaire (FFQ), and physical activity questionnaire. Through demographic questionnaire the age, sex, marital status, level of education, occupation and income level, personal habits including smoking of cigarette, pipe, and hookah and drinking alcohol, and the general characteristics of the individuals were collected. The other part of the questionnaire contained information about medical history of individuals.
Dietary information was collected using a FFQ including 125 food items by face-to-face interview. Participants responded questions about the frequency and amount of food consumed. The validity and reliability of this questionnaire has already been confirmed [
17]. The amount of each food item was based on grams of food consumed per day. According to the reference table that expresses the amount of food antioxidant content in terms of 100 g of foods [
18], the daily amounts of food antioxidants consumed by each person were calculated [
19]. The antioxidant content of foods based on the oxygen radical absorbance capacity (ORAC) method has already been approved by the U.S. Department of Agriculture [
20]; it expresses the degree and duration of inhibition of oxidation induced by proxy radicals and is equivalent to Trolux [
18]. Finally, we categorized participants into tertiles according to total antioxidant capacity (TAC) intake, and considered the lowest group as reference.
Physical activity was assessed using the International Physical Activity Questionnaire-Short Form (IPAQ-SF) which includes seven items related to physical activity during a week. The duration of physical activity was recorded in hours or minutes per day. The data were extracted and used based on metabolic equivalents per hour per week (MET-hour/week). Finally, the results were classified into 3 groups: low, moderate, and severe activity [
21].
Height was measured without shoes by a stadiometer with an accuracy of 0.1 cm. Weight was measured with minimal clothes and without shoes in fasting mode using Camry digital scale (EB9320; Camry, Zhaoqing, China). Waist and hip circumferences were measured with minimum clothes in the standing position using a non-elastic tape at the umbilical area and in the widest part of the pelvis respectively. The waist to hip ratio (WHR) was calculated by dividing the waist circumference to hip circumference. The body mass index (BMI) was obtained by dividing weight (kg) to height squared (m2).
Following 10–12 hours of fasting, 10 mL of venous blood sample (in the first 24 hours of hospitalization) was taken from each participant to evaluate biochemical parameters including lipid profile (total cholesterol [TC], low- and high-density lipoprotein cholesterol [LDL-C and HDL-C], triglycerides [TG]), serum levels of inflammatory markers (IL-17, ICAM, VCAM), and TAC.
Data analysis
The quantitative and qualitative variables are reported as mean ± standard deviation (SD), and number (percentage), respectively. The normality of the data was assessed using the Kolmogorov-Smirnov test. The DTAC was categorized into tertiles. The comparative tests for quantitative and qualitative variables were analysis of variance and χ2, respectively. The Tukey post hoc test was used to compare each group with others. To examine the relationships, univariate and multiple linear regression models were used in which the effect of confounding variables such as age, sex and BMI were adjusted. For all tests, p value less than 0.05 is considered as a statistically significant level. The analyses were performed with STATA 14.2 software (Stata Corp., College Station, TX, USA).
RESULTS
A total of 146 patients undergoing CABG surgery with age of 61.78 ± 10.04 years were evaluated. No significant difference was found among the demographic variables based on DTAC tertiles (p > 0.05). There was no statistically significant difference in the amount of physical activity of the participants by the tertiles of DTAC (p = 0.755) (
Table 1).
Table 1 Distribution of demographic variables among participants based on the DTAC
Table 1
|
Demographic variable |
Frequency (percentage) |
Tertiles of DTAC (μmol TE/100 g) |
p value*
|
T1 (n = 49)
(0.76–2.2) |
T2 (n = 49)
(2.21–3.19) |
T3 (n = 48)
(3.2–14.61) |
|
Age (years) |
146 (100) |
61.32 ± 10.98 |
62.16 ± 10.06 |
61.87 ± 9.22 |
0.917 |
|
Age of disease onset (years) |
146 (100) |
58.16 ± 12.91 |
57.10 ± 12.72 |
58.70 ± 10.36 |
0.800 |
|
Sex |
|
|
|
|
0.178 |
|
Male |
102 (69.86) |
39 (79.59) |
31 (63.27) |
32 (66.67) |
|
Female |
44 (30.14) |
10 (20.41) |
18 (36.73) |
16 (33.33) |
|
Marital status |
|
|
|
|
0.510 |
|
Marriage |
130 (89.04) |
42 (85.71) |
43 (87.76) |
45 (93.75) |
|
Single |
1 (0.68) |
1 (2.04) |
0 (0) |
0 (0) |
|
Widow |
15 (10.27) |
6 (12.24) |
6 (12.24) |
3 (6.25) |
|
Level of education |
|
|
|
|
0.114 |
|
Illiterate |
69 (47.26) |
17 (34.69) |
27 (55.10) |
25 (52.08) |
|
Elementary |
45 (30.83) |
15 (30.61) |
13 (26.53) |
17 (35.42) |
|
High school |
22 (15.07) |
9 (18.37) |
8 (16.33) |
5 (10.42) |
|
University degree |
10 (6.84) |
8 (16.33) |
1 (2.04) |
1 (2.08) |
|
Occupation |
|
|
|
|
0.805 |
|
Housewife |
40 (27.40) |
10 (20.41) |
15 (30.61) |
15 (31.65) |
|
Livestock |
19 (13.01) |
6 (12.24) |
8 (16.33) |
5 (10.42) |
|
Manual worker |
8 (5.48) |
2 (4/08) |
4 (8.16) |
2 (4.17) |
|
Freelance |
35 (23.97) |
12 (24.49) |
10 (20.41) |
13 (27.08) |
|
Employee |
5 (3.42) |
1 (2.04) |
2 (4.08) |
2 (4.17) |
|
Retired |
36 (24.66) |
16 (32.65) |
10 (20.41) |
10 (20.83) |
|
Other |
3 (2.05) |
2 (4.08) |
0 (0) |
1 (2.08) |
|
Income level |
|
|
|
|
0.464 |
|
Weak |
69 (47.26) |
20 (40.82) |
26 (53.06) |
23 (47.92) |
|
Medium |
76 (52.05) |
29 (59.18) |
23 (46.94) |
24 (50) |
|
Financial |
1 (0.68) |
0 (0) |
0 (0) |
1 (2.08) |
|
Smoking |
|
|
|
|
0.312 |
|
Yes |
47 (32.19) |
19 (38.78) |
16 (32/65) |
12 (25) |
|
No |
79 (54.11)) |
27 (55.10) |
25 (51.02) |
27 (56/25) |
|
Exposed |
20 (13.70) |
3 (6.12) |
8 (16.33) |
9 (18.75) |
|
Alcohol consumption |
|
|
|
|
0.236 |
|
Yes |
17 (11.64) |
3 (6.12) |
9 (18.37) |
5 (10.42) |
|
No |
129 (88.35) |
46 (93.88) |
40 (81.63) |
43 (89.58) |
|
Physical activity |
|
|
|
|
0.755 |
|
Low |
84 (57.53) |
26 (53.06) |
29 (59.18) |
29 (60.42) |
|
Moderate |
60 (41.10) |
23 (46.94) |
19 (38.78) |
18 (37.5) |
|
Severe |
2 (1.37) |
0 (0) |
1 (2.04) |
1 (2.08) |
The BMI of patients was 27.0 ± 3.8 kg/m
2 that was not statistically significant among DTAC tertiles (p = 0.249). The mean values of WHR was not significantly different among the antioxidant tertiles (p = 0.664). The mean values of fasting blood glucose (FBG) was 112.1 ± 34.4 mg/dL, which did not show a statistically significant difference among the tertiles (p = 0.757). The mean values of the ICAM and VCAM in all patients were 320.3 ± 288.9 and 271.2 ± 162.4 ng/dL, which were significantly different among the antioxidant tertiles (p < 0.001 for both). serum TAC levels were also significantly different among the tertiles (p = 0.027). The number of obstructive vessels in the first, second and third tertiles of the antioxidant index were 2.94 ± 0.6, 2.88 ± 0.6, and 2.7 ± 0.6, respectively (p = 0.054) (
Table 2).
Table 2 Comparison of mean anthropometric variables, blood pressure and biochemical factors in DTAC tertiles
Table 2
|
Variables |
Average (n = 146) |
Tertiles of DTAC (μmol TE/100 g) |
p value |
Tukey post hoc test |
T1 (n = 49)
(0.76–2.2) |
T2 (n = 49)
(2.21–3.19) |
T3 (n = 48)
(3.2–14.61) |
|
Height (cm) |
164.94 ± 8.56 |
164.94 ± 7.88 |
164.45 ± 8.60 |
164.85 ± 9.32 |
0.955 |
- |
|
Weight (kg) |
72.95 ± 11.02 |
73.81 ± 11.46 |
70.95 ± 10.92 |
74.12 ± 10.61 |
0.296 |
- |
|
BMI (kg/m2) |
27.00 ± 3.83 |
27.10 ± 3.50 |
26.31 ± 4.01 |
27.60 ± 3.87 |
0.249 |
- |
|
Hip circumference (cm) |
94.79 ± 8.49 |
95.10 ± 8.01 |
93.37 ± 7.65 |
95.94 ± 9.66 |
0.316 |
- |
|
Waist circumference (cm) |
103.42 ± 8.74 |
102.97 ± 8.38 |
101.98 ± 9.36 |
105.33 ± 8.27 |
0.153 |
- |
|
WHR |
1.10 ± 0.11 |
1.09 ± 0.10 |
1.09 ± 0.08 |
1.11 ± 0.13 |
0.664 |
- |
|
Energy intake (kcal/day) |
2,439.9 ± 1,351.7 |
2,570.50 ± 1,284.8 |
2,255.3 ± 874.2 |
2,493.1 ± 1,763.8 |
0.489 |
- |
|
FBG (mg/dL) |
112.06 ± 33.42 |
109.67 ± 28.47 |
114.71 ± 42.49 |
111.79 ± 27.85 |
0.757 |
- |
|
LDL-C (mg/dL) |
84.28 ± 25.50 |
89.59 ± 28.54 |
80.69 ± 23.62 |
82.52 ± 23.64 |
0.190 |
- |
|
HDL-C (mg/dL) |
37.32 ± 9.16 |
38.26 ± 10.94 |
36.82 ± 7.54 |
36.89 ± 8.77 |
0.684 |
- |
|
TG (mg/dL) |
130.94 ± 51.74 |
133.73 ± 54.72 |
127.18 ± 50.43 |
131.94 ± 48.48 |
0.813 |
- |
|
TC (mg/dL) |
150.60 ± 37.90 |
157.45 ± 34.14 |
150.10 ± 45.22 |
144.12 ± 32.56 |
0.223 |
- |
|
IL-17(ng/dL) |
44.99 ± 52.12 |
54.24 ± 68.84 |
43.16 ± 49.17 |
37.40 ± 30.35 |
0.271 |
- |
|
ICAM (ng/dL)†
|
320.31 ± 288.90 |
578.58 ± 388.60 |
224.62 ± 66.49 |
165.12 ± 26.88 |
< 0.001*
|
T2 vs. T1, < 0.001 |
|
T3 vs. T1, 0.001 |
|
VCAM (ng/dL) |
271.24 ± 162.36 |
447.12 ± 165.25 |
208.63 ± 51.02 |
155.60 ± 28.02 |
< 0.001*
|
T2 vs. T1, < 0.001 |
|
T3 vs. T1, 0.001 |
|
T3 vs. T2, 0.030 |
|
Serum TAC (ng/dL) |
1.03 ± 0.41 |
0.64 ± 0.30 |
1.06 ± 0.22 |
1.45 ± 0.16 |
0.027*
|
T2 vs. T1, < 0.001 |
|
T3 vs. T1, < 0.001 |
|
T3 vs. T2, < 0.001 |
|
SBP (mmHg) |
128.26 ± 17.44 |
131.23 ± 19.04 |
126.38 ± 16.21 |
127.14 ± 16.91 |
0.336 |
- |
|
Number of obstructive vessels |
2.82 ± 0.57 |
2.94 ± 0.59 |
2.88 ± 0.55 |
2.66 ± 0.59 |
0.054 |
- |
|
Heart rate (number per minute) |
73.57 ± 12.51 |
71.71 ± 12.47 |
75.73 ± 13.65 |
73.27 ± 11.20 |
0.278 |
- |
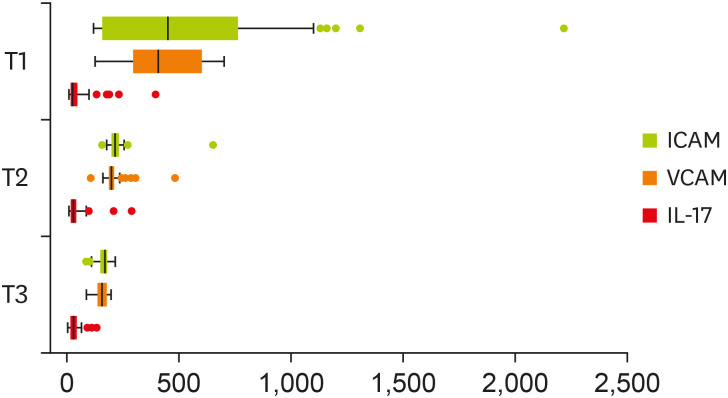
Mean values of inflammatory biomarkers among the DTAC tertiles presented in
Figure 1. As shown in
Table 3 the linear regression analysis in the crude and adjusted models indicated that the mean β values of TG (mg/dL) in the third tertile of DTAC was −1.8 (p = 0.865) and −3.6 (p = 0.734) respectively, which were lower than that in the first tertile, but did not reach the statistically significant. The mean values of IL-17 (ng/dL) in the second and third tertile of DTAC were lower than that of the first tertile, but did not reach the statistical significance (p = 0.113 and p = 0.144, respectively). the mean values of ICAM (ng/dL) in the second and third tertiles were lower compared to the first tertile (p < 0.001 for both comparisons). This association remained significant after adjustment of potentially confounding variables. The mean values of the VCAM (ng/dL) in the second and third tertiles were lower than the first tertile (p < 0.001 for both comparisons), and the statistical significance were retained after the adjustment. In the crude model, the mean values of serum TAC (ng/dL) in the second and third tertiles of the DTAC were significantly higher than that in the first tertile (p < 0.001 for both). This association remained significant after the adjustment of confounding variables (
Table 3).
Figure 1
Mean values of inflammatory biomarkers among the DTAC tertiles.
Values are expressed as mean ± standard deviation.
DTAC, dietary total antioxidant capacity; IL-17, interleukine17; ICAM, intercellular adhesion molecule; VCAM, vascular cells adhesion molecule.
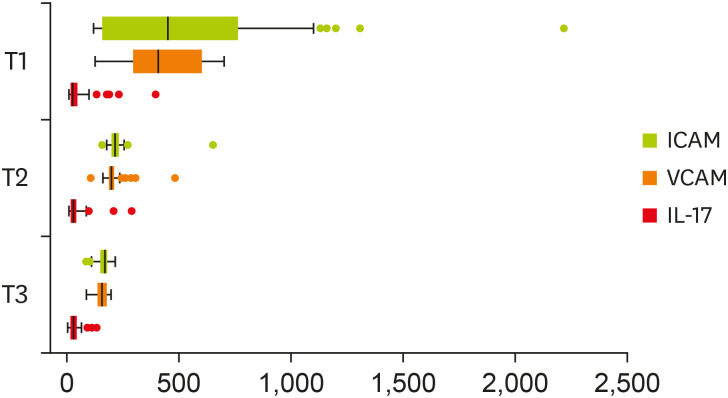
Table 3 Relationship between DTAC and studied variables in patients undergoing surgery coronary artery bypass graft
Table 3
|
Variable |
Regression model |
Tertiles of DTAC (μmol TE/100 g) |
T1 (n = 49)
(0.76–2.2) |
T2 (n = 49)
(2.21–3.19) |
p value*
|
T3 (n = 48)
(3.2–14.61) |
p value†
|
|
References |
β (95% CI) |
β (95% CI) |
|
Weight (kg) |
Crude model |
0 |
−2.80 (−7.21, 1.52) |
0.202 |
0.31 (−4.10, 4.71) |
0.887 |
|
Adjusted model |
0 |
−1.61 (−5.62, 2.32) |
0.383 |
−1.20 (−2.81, 5.33) |
0.535 |
|
Waist circumference (cm) |
Crude model |
0 |
−1.00 (−4.40, 2.41) |
0.570 |
2.31 (−1.10, 5.81) |
0.184 |
|
Adjusted model |
0 |
0.58 (−1.35, 2.53) |
0.552 |
1.41 (−0.56, 3.30) |
0.163 |
|
WHR |
Crude model |
0 |
0.004 (−0.04, 0.04) |
0.837 |
0.02 (−0.02, 0.06) |
0.387 |
|
Adjusted model |
0 |
0.0004 (−0.04, 0.04) |
0.631 |
0.02 (−0.02, 0.06) |
0.504 |
|
FBG (mg/dL) |
Crude model |
0 |
5.04 (−8.37, 18.45) |
0.459 |
2.12 (−11.43, 15.60) |
0.757 |
|
Adjusted model |
0 |
5.74 (−7.84, 19.32) |
0.405 |
1.38 (−12.09, 14.85) |
0.840 |
|
HDL-C (mg/dL) |
Crude model |
0 |
−1.44 (−5.11, 2.22) |
0.439 |
−1.36 (−5.04, 2.33) |
0.467 |
|
Adjusted model |
0 |
−2.34 (−6.02, 1.35) |
0.212 |
−1.91 (−5.56, 1.74) |
0.303 |
|
TG (mg/dL) |
Crude model |
0 |
−6.55 (−27.33, 14.22) |
0.534 |
−1.80 (−22.68, 19.09) |
0.865 |
|
Adjusted model |
0 |
−6.33 (−27.39, 14.72) |
0.553 |
−3.60 (−24.49, 17.29) |
0.734 |
|
TC (mg/dL) |
Crude model |
0 |
−7.35 (−22.43, 7.73) |
0.337 |
−13.32 (−28.48, 1.83) |
0.084 |
|
Adjusted model |
0 |
−11.61 (−26.71, 3.49) |
0.131 |
−14.51 (−29.50, 0.49) |
0.172 |
|
LDL-C (mg/dL) |
Crude model |
0 |
−8.90 (−19.03, 1.24) |
0.085 |
−7.07 (−17.26, 3.12) |
0.172 |
|
Adjusted model |
0 |
−10.13 (−20.52, 0.25) |
0.056 |
−7.88 (−18.17, 2.43) |
0.113 |
|
IL-17 (ng/dL) |
Crude model |
0 |
−11.08 (−31.85, 9.69) |
0.294 |
−16.84 (−37.72, 4.03) |
0.113 |
|
Adjusted model |
0 |
−10.94 (−31.97, 10.09) |
0.305 |
−15.50 (−36.36, 5.35) |
0.144 |
|
ICAM (ng/dL) |
Crude model |
0 |
−353.96 (−455.13, −262.78) |
< 0.001 |
−413.45 (−505.10, −321.81) |
< 0.001 |
|
Adjusted model |
0 |
−359.6 (−453.1, −266.1) |
< 0.001 |
−417.18 (−509.86, −324.50) |
< 0.001 |
|
VCAM (ng/dL) |
Crude model |
0 |
−238.49 (−279.02, −197.42) |
< 0.001 |
−291.52 (−332.25, −250.78) |
< 0.001 |
|
Adjusted model |
0 |
−238.84 (−280.27, −197.42) |
< 0.001 |
−293.25 (−334.34, −252.16) |
< 0.001 |
|
Serum TAC (ng/dL) |
Crude model |
0 |
0.47 (0.38, 0.56) |
< 0.001 |
0.85 (0.76, 0.94) |
< 0.001 |
|
Adjusted model |
0 |
0.47 (0.38, 0.56) |
< 0.001 |
0.86 (0.77, 0.95) |
< 0.001 |
|
SBP (mmHg) |
Crude model |
0 |
−4.85 (−11.8, 2.11) |
0.170 |
−4.09 (−11.09, 2.90) |
0.249 |
|
Adjusted model |
0 |
−5.21 (−12.14, 1.79) |
0.143 |
−4.65 (−11.55, 2.24) |
0.185 |
|
Heart rate (number per minute) |
Crude model |
0 |
4.02 (−0.96, 9.01) |
0.113 |
1.55 (−3.46, 6.56) |
0.540 |
|
Adjusted model |
0 |
3.65 (−1.33, 8.64) |
0.150 |
0.77 (−4.18, 5.72) |
0.758 |
|
Number of obstructive vessels |
Crude model |
0 |
−0.08 (−0.3, 0.14) |
0.475 |
−0.27 (−0.49, −0.05) |
0.119 |
|
Adjusted model |
0 |
−0.06 (−0.3, −0.17) |
0.605 |
−0.24 (−0.47, −0.02) |
0.134 |
DISCUSSION
The findings of this study showed that patients undergoing CABG surgery showed significant correlation of the increased DTAC with the increased antioxidant and decreased ICAM and VCAM levels in serum, although statistically significant association between the IL-17 and DTAC was not observed. Meta-analysis studies by Aune et al. [
22,
23,
24] showed a direct correlation between DTAC and serum antioxidant levels in individuals with cancer and CVDs. On the other hand, the cohort studies have reported an inverse relationship between serum antioxidant levels and the prevalence of breast cancer [
25,
26]. The positive effects of antioxidants on reducing the level of adhesion molecules have also been confirmed in clinical trial studies; antioxidant supplementation is usually associated with a reduction in the level of free radicals such as superoxide which in turn inhibits the tumor necrosis factor (TNF)-α signaling pathway and reduces the level of LDL oxidation that are the main factors in stimulating the secretion of adhesion molecules [
27].
It has been indicated that dietary antioxidants can reduce the secretion of inflammatory biomarkers such as IL-6, CRP, and adhesion molecules by inhibiting the activity of the nuclear factor-κB pathway [
28,
29]. The study of Mena et al. [
30] showed that Mediterranean diets, which have a high antioxidant content reduces the secretion of IL-6, CRP, ICAM, and VCAM. In a cohort study with a 15-year follow-up on two black and white races performed by Sijtsma et al. [
12], the level of adhesion molecules was much lower in the group who consumed fruits and vegetables than the counterpart. In addition, Lopez-Garcia et al. [
31] reported that circulating ICAM levels were directly related to the Western diet and inversely related to the Mediterranean diet. To our knowledge, no study has directly examined the association between DTAC and serum IL-17 levels. It can be said that we can attenuate inflammatory conditions and accordingly reduce cardiovascular complications by changing people's diet with food components rich in antioxidants.
In the present study, no significant relationship was observed between DTAC and anthropometric indices. Some studies have reported an inverse relationship between DTAC and anthropometric indices, while some others have shown the lack of such a correlation [
32,
33,
34]. It has been imagined that inflammatory condition is the consequence of oxidative stress dominance over antioxidant defenses, and insufficient consumption of antioxidant sources can induce obesity [
6,
32,
33]. Some studies have also reported that exposure to reactive oxygen species (ROS) stimulates the differentiation and proliferation of fat cells, and the excess fat leads to the production of more ROS; this vicious cycle exacerbates obesity and increases the likelihood of CVDs [
35,
36]. Considering the caloric intake of the patients in our study ranged from 2,000 to 3,000 kcal per day and significant difference was not found in their physical activity, the lack of a significant relationship between DTAC and anthropometric indices can be justifiable. The differences in the sample size, age group, race and population may be other causes of these discrepancies because some of these studies have been performed in the healthy individuals.
The findings of this study showed that DTAC was not significantly associated with lipid profiles (TC, TG, LDL-C, and HDL-C) and FBG. In the study conducted by Georgoulis et al. [
37], no correlation was found between DTAC and lipid profile. A study on healthy Brazilian youths showed an inverse relationship between DTAC and lipid profile [
33]. Other studies in Iran and the United States have shown that the level of lipid profile has also increased with increasing DTAC [
1,
32,
33]. In addition to differences in sample size and the reporting errors in the FFQ, the reason for the differences can be mainly due to the differences in the characteristics of studied populations, so that most significant relationships have been reported in studies including the population with no history of chronic disease and accordingly without use of specific therapies. However, the participants in the present study were patients and those mostly treated with lipid lowering drugs. Some studies have reported inverse relationship between DTAC with FBG and homeostasis model assessment-estimated insulin resistance, and some others have proven lack of such a relationship [
1,
6,
32,
34]. In one study, a correlation was found between a diet rich in antioxidants and the prevalence of diabetes [
38]. A noteworthy point in stating the cause of these discrepancies is that some diabetics were also included in studies that reported an inverse relationship between DTAC and FBG, but diabetic patients were excluded in our study.
The results of the present study did not show a relationship between DTAC and IL-17 levels. To date, no study has directly examined the relationship between DTAC and IL-17 levels. This molecule plays a role in controlling inflammation and even the secretion of other inflammatory cytokines [
39]. Also, it has a key role in the atherosclerotic process by increasing the expression of adhesion molecules, stimulating monocytes, and increasing the adhesion of macrophages to the vascular, as well as increasing the likelihood of LDL oxidation [
8,
9].
Our findings showed no association between DTAC with systolic blood pressure, heart rate, and number of blocked arteries. The results of the study done by Kim et al. [
4] on American adults were in line with the present study. Several studies have shown an inverse relationship between DTAC and blood pressure [
6,
32,
40]. The main cause of the discrepancies can be considered as differences in the studied populations. In studies that reported an inverse relationship between DTAC and blood pressure, the subjects were healthy with no history of chronic diseases; however, the participants of our study mostly suffered from hypertension and were treated with antihypertensive and cardiac drugs.
This cross-sectional study included only a small number of CABG candidates (n = 146). Considering the clinical and emergency conditions of the participants in the present study, a large number of patients could not be included to the study. Also, due to the dependence of the FFQ on memory, reporting errors in completing the FFQ can be inevitable. However, one of the strengths of the present study is the simultaneous investigation of several inflammatory and biochemical factors in patients undergoing CABG surgery.
CONCLUSION
The present study showed that increased DTAC was significantly associated with increased antioxidant and decreased serum concentrations of ICAM and VCAM in candidates for CABG surgery. Considering the role of these factors in the regulation of inflammatory processes, these findings indicate the importance of dietary antioxidants in coronary artery diseases. It seems that consumption of diet containing antioxidant compounds in people with coronary artery diseases along with medication may be useful. To assess this relationship in detail, it is necessary to conduct studies in particular clinical trials with a large sample size.
NOTES
-
Funding: Deputy for Research and Technology of Kermanshah University of Medical Sciences, Kermanshah, Iran was funded (No. 990108) this study.
-
Conflict of Interest: The authors declare that they have no competing interests.
ACKNOWLEDGEMENTS
Authors thank all those who participated in this study.
REFERENCES
- 1. Bahadoran Z, Mirmiran P, Tohidi M, Azizi F. Longitudinal associations of high-fructose diet with cardiovascular events and potential risk factors: Tehran Lipid and Glucose Study. Nutrients 2017;9:872.
- 2. Ghorbaninejad P, Mohammadpour S, Djafari F, Tajik S, Shab-Bidar S. Dietary total antioxidant capacity and its association with renal function and progression of chronic kidney disease in older adults: a report from a developing country. Clin Nutr Res 2020;9:296-306.
- 3. Jamee Shahwan A, Abed Y, Desormais I, Magne J, Preux PM, Aboyans V, Lacroix P. Epidemiology of coronary artery disease and stroke and associated risk factors in Gaza community - Palestine. PLoS One 2019;14:e0211131.
- 4. Kim K, Vance TM, Chun OK. Greater total antioxidant capacity from diet and supplements is associated with a less atherogenic blood profile in US adults. Nutrients 2016;8:15.
- 5. Rasaee S, Alizadeh M, Kheirouri S, Abdollahzad H. Does total antioxidant capacity affect the features of metabolic syndrome? A systematic review. Nutr Food Sci 2020;51:100-113.
- 6. Puchau B, Zulet MA, de Echávarri AG, Hermsdorff HH, Martínez JA. Dietary total antioxidant capacity is negatively associated with some metabolic syndrome features in healthy young adults. Nutrition 2010;26:534-541.
- 7. Mozaffari H, Daneshzad E, Surkan PJ, Azadbakht L. Dietary total antioxidant capacity and cardiovascular disease risk factors: a systematic review of observational studies. J Am Coll Nutr 2018;37:533-545.
- 8. Kim JD, Lee SH, Seo EH, Woo SY, Kim SH, Chung SM, Kim HJ. Role of Th1 and Th17 cells in the development and complexity of coronary artery disease: comparison analysis by the methods of flow cytometry and SYNTAX score. Coron Artery Dis 2015;26:604-611.
- 9. Park H, Li Z, Yang XO, Chang SH, Nurieva R, Wang YH, Wang Y, Hood L, Zhu Z, Tian Q, Dong C. A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17. Nat Immunol 2005;6:1133-1141.
- 10. Malik I, Danesh J, Whincup P, Bhatia V, Papacosta O, Walker M, Lennon L, Thomson A, Haskard D. Soluble adhesion molecules and prediction of coronary heart disease: a prospective study and meta-analysis. Lancet 2001;358:971-976.
- 11. Luc G, Arveiler D, Evans A, Amouyel P, Ferrieres J, Bard JM, Elkhalil L, Fruchart JC, Ducimetiere P. PRIME Study Group. Circulating soluble adhesion molecules ICAM-1 and VCAM-1 and incident coronary heart disease: the PRIME study. Atherosclerosis 2003;170:169-176.
- 12. Sijtsma FP, Meyer KA, Steffen LM, Van Horn L, Shikany JM, Odegaard AO, Gross MD, Kromhout D, Jacobs DR Jr. Diet quality and markers of endothelial function: the CARDIA study. Nutr Metab Cardiovasc Dis 2014;24:632-638.
- 13. Wang TK, Woodhead A, Ramanathan T, Pemberton J. Relationship between diabetic variables and outcomes after coronary artery bypass grafting in diabetic patients. Heart Lung Circ 2017;26:371-375.
- 14. Wang Y, Chun OK, Song WO. Plasma and dietary antioxidant status as cardiovascular disease risk factors: a review of human studies. Nutrients 2013;5:2969-3004.
- 15. Hedman A, Larsson PT, Alam M, Wallen NH, Nordlander R, Samad BA. CRP, IL-6 and endothelin-1 levels in patients undergoing coronary artery bypass grafting. Do preoperative inflammatory parameters predict early graft occlusion and late cardiovascular events? Int J Cardiol 2007;120:108-114.
- 16. Kolarzyk E, Pietrzycka A, Zając J, Morawiecka-Baranek J. Relationship between dietary antioxidant index (DAI) and antioxidants level in plasma of Kraków inhabitants. Adv Clin Exp Med 2017;26:393-399.
- 17. Moradi S, Pasdar Y, Hamzeh B, Najafi F, Nachvak SM, Mostafai R, Niazi P, Rezaei M. Comparison of 3 nutritional questionnaires to determine energy intake accuracy in Iranian adults. Clin Nutr Res 2018;7:213-222.
- 18. Haytowitz DB, Bhagwat S. USDA database for the oxygen radical absorbance capacity (ORAC) of selected foods, release 2. Beltsville (MD): U.S. Department of Agriculture; 2010. p. 10-48.
- 19. Mirmiran P, Bahadoran Z, Ghasemi A, Azizi F. Contribution of dietary amino acids composition to incidence of cardiovascular outcomes: a prospective population-based study. Nutr Metab Cardiovasc Dis 2017;27:633-641.
- 20. Harasym J, Oledzki R. Effect of fruit and vegetable antioxidants on total antioxidant capacity of blood plasma. Nutrition 2014;30:511-517.
- 21. Ahmadi E, Abdollahzad H, Pasdar Y, Rezaeian S, Moludi J, Nachvak SM, Mostafai R. Relationship between the consumption of milk-based oils including butter and Kermanshah ghee with metabolic syndrome: Ravansar Non-Communicable Disease cohort study. Diabetes Metab Syndr Obes 2020;13:1519-1530.
- 22. Aune D, Chan DS, Lau R, Vieira R, Greenwood DC, Kampman E, Norat T. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ 2011;343:d6617.
- 23. Aune D, Giovannucci E, Boffetta P, Fadnes LT, Keum N, Norat T, Greenwood DC, Riboli E, Vatten LJ, Tonstad S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol 2017;46:1029-1056.
- 24. Aune D, Keum N, Giovannucci E, Fadnes LT, Boffetta P, Greenwood DC, Tonstad S, Vatten LJ, Riboli E, Norat T. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Am J Clin Nutr 2018;108:1069-1091.
- 25. Eliassen AH, Hendrickson SJ, Brinton LA, Buring JE, Campos H, Dai Q, Dorgan JF, Franke AA, Gao YT, Goodman MT, Hallmans G, Helzlsouer KJ, Hoffman-Bolton J, Hultén K, Sesso HD, Sowell AL, Tamimi RM, Toniolo P, Wilkens LR, Winkvist A, Zeleniuch-Jacquotte A, Zheng W, Hankinson SE. Circulating carotenoids and risk of breast cancer: pooled analysis of eight prospective studies. J Natl Cancer Inst 2012;104:1905-1916.
- 26. Zhang X, Spiegelman D, Baglietto L, Bernstein L, Boggs DA, van den Brandt PA, Buring JE, Gapstur SM, Giles GG, Giovannucci E, Goodman G, Hankinson SE, Helzlsouer KJ, Horn-Ross PL, Inoue M, Jung S, Khudyakov P, Larsson SC, Lof M, McCullough ML, Miller AB, Neuhouser ML, Palmer JR, Park Y, Robien K, Rohan TE, Ross JA, Schouten LJ, Shikany JM, Tsugane S, Visvanathan K, Weiderpass E, Wolk A, Willett WC, Zhang SM, Ziegler RG, Smith-Warner SA. Carotenoid intakes and risk of breast cancer defined by estrogen receptor and progesterone receptor status: a pooled analysis of 18 prospective cohort studies. Am J Clin Nutr 2012;95:713-725.
- 27. Vincent HK, Bourguignon CM, Weltman AL, Vincent KR, Barrett E, Innes KE, Taylor AG. Effects of antioxidant supplementation on insulin sensitivity, endothelial adhesion molecules, and oxidative stress in normal-weight and overweight young adults. Metabolism 2009;58:254-262.
- 28. Kobayashi S, Murakami K, Sasaki S, Uenishi K, Yamasaki M, Hayabuchi H, Goda T, Oka J, Baba K, Ohki K, Watanabe R, Sugiyamama Y. Dietary total antioxidant capacity from different assays in relation to serum C-reactive protein among young Japanese women. Nutr J 2012;11:91.
- 29. Brasier AR, Innes KE, Vincent KR. The nuclear factor-κB–interleukin-6 signalling pathway mediating vascular inflammation. Cardiovasc Res 2010;86:211-218.
- 30. Mena MP, Sacanella E, Vazquez-Agell M, Morales M, Fitó M, Escoda R, Serrano-Martínez M, Salas-Salvadó J, Benages N, Casas R, Lamuela-Raventós RM, Masanes F, Ros E, Estruch R. Inhibition of circulating immune cell activation: a molecular antiinflammatory effect of the Mediterranean diet. Am J Clin Nutr 2009;89:248-256.
- 31. Lopez-Garcia E, Rodriguez-Artalejo F, Li TY, Fung TT, Li S, Willett WC, Rimm EB, Hu FB. The Mediterranean-style dietary pattern and mortality among men and women with cardiovascular disease. Am J Clin Nutr 2014;99:172-180.
- 32. Bahadoran Z, Golzarand M, Mirmiran P, Shiva N, Azizi F. Dietary total antioxidant capacity and the occurrence of metabolic syndrome and its components after a 3-year follow-up in adults: Tehran Lipid and Glucose Study. Nutr Metab (Lond) 2012;9:70.
- 33. Hermsdorff HH, Puchau B, Volp AC, Barbosa KB, Bressan J, Zulet MÁ, Martínez JA. Dietary total antioxidant capacity is inversely related to central adiposity as well as to metabolic and oxidative stress markers in healthy young adults. Nutr Metab (Lond) 2011;8:59.
- 34. Kim K, Vance TM, Chen MH, Chun OK. Dietary total antioxidant capacity is inversely associated with all-cause and cardiovascular disease death of US adults. Eur J Nutr 2018;57:2469-2476.
- 35. Lee H, Lee YJ, Choi H, Ko EH, Kim JW. Reactive oxygen species facilitate adipocyte differentiation by accelerating mitotic clonal expansion. J Biol Chem 2009;284:10601-10609.
- 36. Sen S, Simmons RA. Maternal antioxidant supplementation prevents adiposity in the offspring of Western diet-fed rats. Diabetes 2010;59:3058-3065.
- 37. Georgoulis M, Fragopoulou E, Kontogianni MD, Margariti A, Boulamatsi O, Detopoulou P, Tiniakos D, Zafiropoulou R, Papatheodoridis G. Blood redox status is associated with the likelihood of nonalcoholic fatty liver disease irrespectively of diet's total antioxidant capacity. Nutr Res 2015;35:41-48.
- 38. Hamer M, Chida Y. Intake of fruit, vegetables, and antioxidants and risk of type 2 diabetes: systematic review and meta-analysis. J Hypertens 2007;25:2361-2369.
- 39. Gong F, Liu Z, Liu J, Zhou P, Liu Y, Lu X. The paradoxical role of IL-17 in atherosclerosis. Cell Immunol 2015;297:33-39.
- 40. Farvid MS, Homayouni F, Kashkalani F, Shirzadeh L, Valipour G, Farahnak Z. The associations between oxygen radical absorbance capacity of dietary intake and hypertension in type 2 diabetic patients. J Hum Hypertens 2013;27:164-168.